


OVERVIEW
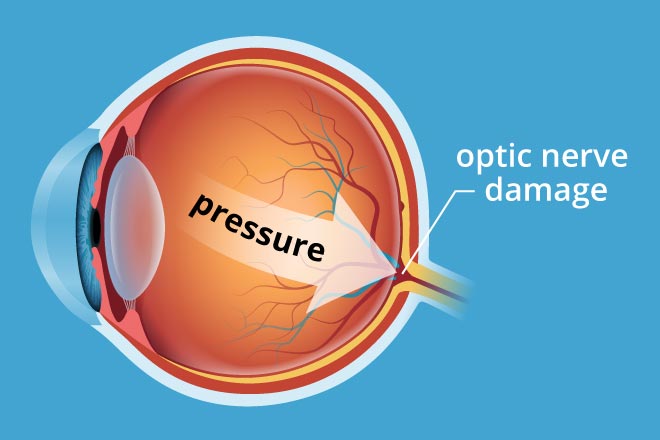
Glaucoma is a serious and rare condition of the eye where the optic nerve is damaged, resulting in the loss of side or peripheral vision, tunnel vision, and blindness. In a normal eye, there is a small anterior chamber filled with clear fluid called aqueous humor. This fluid flows out of an open angle (drainage angle) between the iris (colored portion of the eyeball) and the cornea. At the open angle, the fluid flows out of the eye through a spongy network. If there is a reduction in the flow of fluid at this position, it raises the pressure in the eye, called intraocular pressure (IOP), damages the optic nerve, and causes glaucoma. Glaucoma can affect both eyes. For effective treatment and care, it is crucial to consult the Best Glaucoma Hospital in Rohtak, where experienced specialists and advanced technology ensure the best possible outcomes for patients.
Optic nerve is a bundle of nerve fibers that carries signals from the retina of the eye to the brain, which are processed as images. Damage to the optic nerve cannot be reversed. Hence, there is no cure for glaucoma as the lost vision cannot be restored. However, early diagnosis and detection can preserve your vision and prevent vision loss. For the best care and treatment, it is essential to consult the Best Glaucoma Hospital in Rohtak, where advanced diagnostic tools and expert medical professionals can help manage the condition effectively.
Types of Glaucoma
Primary Open-angle glaucoma : This happens when the meshwork at the drainage angle is unable to drain the aqueous humor effectively. There are no symptoms to begin with except blank or black spots in the vision. However, by the time blank spots become evident in day-to-day activities, there has been considerable damage to the optic nerve. The damage to optic nerve occurs at different IOPs for different individuals. Your ophthalmologist or eye specialist will determine your target IOP and help your maintain it. Often raised IOPs are missed at the first eye pressure testing. However, routine eye pressure testing by trained ophthalmologist can often diagnose this early.
Normal-tension glaucoma : The normal eye pressure is about 21 mm Hg. However, some people suffer an optic damage at 21 mm Hg or pressures below 21 mm Hg. This is called normal tension glaucoma. This is treated just like open angle glaucoma and occurs because for these individuals the target IOP is low. It presents with blind spots in the field of vision.
Closed-angle glaucoma (Angle-closure glaucoma or Narrow-angle glaucoma) : This happens when the iris blocks the flow of aqueous humor. The IOP rises very fast. Individuals with farsightedness (hyperopia) or those of Asian descent are at higher risk for developing this type of glaucoma.
Causes
Symptoms
The signs and symptoms differ with the type of glaucoma. However, there are no signs and symptoms in the early stages of glaucoma. Thereafter, a person may develop black spots in vision, loss of peripheral vision, colored halos, see rainbow colors, have headaches, and develop tunnel vision or blindness. If you or a loved one is experiencing any of these symptoms, it is crucial to seek expert care at the Best Glaucoma Hospital in Rohtak for timely diagnosis and effective treatment. Early intervention can help prevent further vision loss and improve quality of life.
Diagnosis
Since glaucoma does not present with early signs and symptoms, it is detected through a detailed eye examination that includes the following tests at the Best Glaucoma Hospital in Rohtak:
Visual acuity test: Your doctor will ask you to read a chart at different distances to assess how clearly you can see the alphabets.
Visual field test measures: Your doctor will use a special instrument called a perimeter to check your peripheral or side vision. Only one eye is checked at a time, and the other eye is covered with a black patch. In a sitting position, you will be asked to focus straight ahead at a target. A computer will generate noises and send out flashes of light in every direction. Some noises are not accompanied by a flash of light. You will be asked to press a button when you see a flash of light. Your doctor may perform this test every six to twelve months to monitor the change.
Dilated eye exam or Ophthalmoscopy: Your doctor will put some eye drops into your eyes and ask you to wait for some time with your eyes closed. This will help dilate your pupils. One eye is tested at a time. Your eye specialist will use a special magnifying glass (ophthalmoscope) to look into your eyes to examine the retina and the optic nerve. In glaucoma, the nerve fibers of the optic nerve are damaged and cause cupping of the optic nerve. This cupping of the optic nerve causes blank spots in your vision. After the eye examination, your near vision may remain blurred for some hours, so you will not be able to drive back home.
Tonometry: Your doctor will use a special instrument (tonometer) to measure the IOP. Your doctor will put some eye drops to numb the white of your eyes. One eye is tested at a time. The instrument will then be placed on the white of the eye to take the eye pressure. Normal IOP varies between 10 and 21 mm Hg, and is generally around 21mmHg for most eyes.
Pachymetry: Your doctor will put some eye drops to numb your eyes. One eye is tested at a time. A special instrument is then used to measure the thickness of your cornea. Your eye care professional uses an ultrasonic wave instrument to measure the thickness of your cornea.
Gonioscopy: Your doctor will use a mirrored lens to inspect the drainage angle of your eye. One eye is tested at a time. If the drainage angle is not working well, then it is an open-angle glaucoma; if the angle is partially closed, it is closed-angle glaucoma; if the iris completely blocks the angle, it is a dangerous variety of closed-angle glaucoma.
For comprehensive glaucoma care and advanced diagnostic services, visit the Best Glaucoma Hospital in Rohtak to ensure your eye health is in expert hands.
Treatment
Glaucoma can be treated with medicines and surgery. If you are looking for the Best Glaucoma Hospital in Rohtak, it is essential to choose a facility that offers advanced treatments and expert care for glaucoma management.
Glaucoma Medication:
Your doctor will prescribe eye drops to lower your eye pressure. The drops either slow down the formation of aqueous humor or improve its drainage at the drainage angle. You will need to use the eye drops daily, in the dose prescribed by the doctor. It is also important to inform your doctor about all the medications and supplements you are taking, as some drugs can worsen glaucoma.
Glaucoma Surgery:
At the Best Glaucoma Hospital in Rohtak, your doctor will perform different types of surgeries to improve the drainage of aqueous humor. The different surgeries include:
- Laser Trabeculoplasty:
This is typically used to treat open-angle glaucoma. There are two types:- ALT (Argon Laser Trabeculoplasty): The doctor uses a laser to make tiny burns at regular intervals in the trabecular meshwork at the drainage angle, improving its drainage function.
- SLT (Selective Laser Trabeculoplasty): The laser targets specific cells in the meshwork to lower intraocular pressure (IOP). SLT uses lower energy and shorter laser spurts compared to ALT.
Nearly half of the patients undergoing trabeculoplasty may develop increased eye pressure within five years. Repeat trabeculoplasty can be performed in some cases, while most patients rely on eye drops to maintain low eye pressure.
- Laser Iridotomy:
This surgery is recommended for closed-angle glaucoma, where the drainage angle has become very narrow. The doctor uses a laser to create a small hole in the upper part of the iris to improve the flow of aqueous humor. - Peripheral Iridectomy:
If laser iridotomy is ineffective or unlikely to benefit the patient, the doctor may perform a peripheral iridectomy. A small piece of the iris is removed to improve the flow of aqueous humor. This procedure is less common, as most closed-angle glaucoma cases can be treated with medications or laser iridotomy. - Trabeculectomy:
In this procedure, the doctor creates a small flap in the sclera (white coat of the eye) and forms a new drainage channel for the aqueous humor. A filtration reservoir is created under the conjunctiva (the membrane covering the white of the eye). The reservoir, which looks like a small bump, is usually covered by the upper eyelid. The aqueous humor drains through the flap and collects in the reservoir.
For comprehensive glaucoma care, including advanced medications and surgical options, visit the Best Glaucoma Hospital in Rohtak to ensure the best possible outcomes for your eye health.